Annual Quality Account 2025-2026
Date published: 7 July 2026
Summary
Welcome to the East of England Ambulance Service NHS Trust (EEAST) Quality Account for 2025/26. This document has been approved by the Trust Board and is an accurate account of the level of quality of service provided to patients. In developing this Quality Account, we have set out a summary of achievements for 2025/26 and goals for 2026/27 as mandated within the regulatory guidance.
In this report
- Part One
- Foreword and statement on quality from the Board
- Welcome to the East of England Service NHS Trust (EEAST) quality account
- Introducing EEAST's quality account
- What is a Quality Account and what does it mean to EEAST and the people we serve?
- Our current quality position
- Care Quality Commission (CQC)
- Department of Health core quality indicators
- NHS Number and General Medical Practice code validity
- NHS clinical coding error rate
- Data quality
- Data security protection toolkit
- Statement of Accountability
- Part Two
- Quality improvement initiatives
- Priority One - Patient safety
- Priority Two - Clinical effectiveness
- Priority Three - Patient experience
- Part Three
- Progress on the quality account priorities 2025/26
- Performance of the Trust against quality metrics
- Achievements against local priorities set for 2025/26
- Clinical Audit
- Participation in research
- Patient safety incidents
- Patient safety events
- When things go wrong
- Duty of Candour
- National Patient Safety Alerts
- Patient experience and feedback
- Patient and Public Involvement
- Statement from our Community Engagement Group
- Raising concerns and Freedom to Speak Up
- Working with our local communities
- Achievements in 2025/26
- Commissioning for Quality and Innovation (CQuIN)
- Quality success throughout the year
- Quality Governance Committee Assurance
- Statements from the Commissioners, HealthWatch and Overview and Scrutiny Committees
- Glossary
What is a Quality Account and what does it mean to EEAST and the people we serve?
A Quality Account is a mandatory report about the quality of services an NHS healthcare trust provides and is required to be completed in line with the Health and Social Care Act 2012.
Quality reports and accounts are set against the framework of three overlapping key themes, patient safety, clinical effectiveness and patient experience, which can be used to define quality of care.
The content is defined by NHS England and includes outcome results against specific indicators under five headings:
- Preventing people from dying prematurely.
- Enhancing quality of life for people with long term conditions.
- Helping people to recover from episodes of ill health or following injury.
- Ensuring that people have a positive experience of care.
- Treating and caring for people in a safe environment and protecting them from avoidable harm.
In addition to information provided within this report, our newly published Corporate Strategy 2025/30 details what we are aiming to achieve over the next five years and how we are going to do this.
Performance of the Trust against quality metrics
Response Times
Ambulance services are monitored against response times for a Category 1 – 4 system (determined by clinical condition/emergency), with varying response times for each category. The table below summarises the Trust’s performance against the national response time standards for 2025/26 and the improvement seen for each category when compared to the previous year.
| Category | Definition | National standard | Average EEAST Performance 2024/25 and 2025/26 | Improvement |
|---|---|---|---|---|
| C1 | Immediately life-threatening injuries and illnesses. | 7 minutes mean response time | 00:09:08 and 00:08:41 | 00:00:27 |
| 15 minutes 90th centile response time | 00:17:12 and 00:16:16 | 00:00:56 | ||
| C2 | Emergency. | 18 minutes mean response time | 00:42:49 and 00:35:48 | 00:07:01 |
| 40 minutes 90th centile response time | 01:32:50 and 01:15:08 | 00:17:42 | ||
| C3 | Urgent calls and in some instances where patients may be treated in-situ (e.g., their own home) or referred to a different pathway of care. | 120 minutes (2 hours) 90th centile response time | 02:21:56 and 01:55:52 | 00:26:04 |
| C4 | Less urgent. In some instances, patients may be given advice over the phone or referred to another service such as a GP or pharmacist. | 180 minutes (3 hours) 90th centile response time | 03:54:56 and 02:40:32 | 01:14:24 |
- Category C1 maintained a stable performance throughout the year, ranging from a fastest monthly average of 8 minutes 09 seconds to a slowest of 9 minutes 14 seconds. The year-end mean of 00:08:41 reflects an improvement on the previous year’s performance.
- Category C2 experienced greater month-to-month variation, reaching a peak of 00:47:04 in January. Despite this fluctuation a year-end mean response time of 00:35:48 was achieved which is also an improvement on the previous year.
- Category C3 recorded response times ranging from 01:21:10 to 02:41:42, with a year-end mean of 01:55:52, also representing improvement on the previous year.
- Category C4 continued to show the longest response times, ending the year with a mean of 02:40:32. However, this is also an improvement on the previous year’s performance.
Category 1 performance July 2024 - January 2026
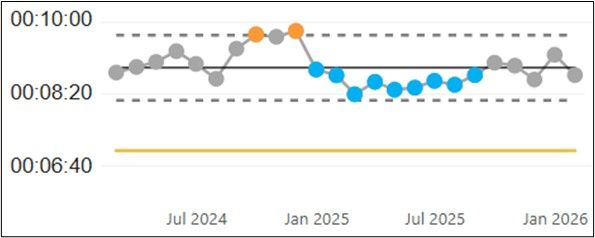
Graph summary: Data points in grey, orange, and blue fluctuate around a central target line at approximately 8 minutes 20 seconds. Two points in late 2024 exceed the upper dashed limit near 10 minutes, while several points in early 2025 drop below the lower dashed limit. Performance stabilises near the target line through mid to late 2025.
Category 2 performance July 2024 - January 2026
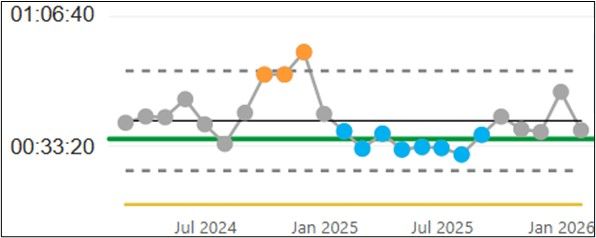
Graph summary: Line chart showing time performance from July 2024 to January 2026 with a central green target line at approximately 33 minutes 20 seconds and dashed upper and lower limits. Grey data points fluctuate around the target in 2024. Three orange points in late 2024 and early 2025 rise above the upper limit, peaking at around 1 hour 6 minutes. In early to mid 2025, several blue points fall below the lower limit before gradually returning toward the target by late 2025.
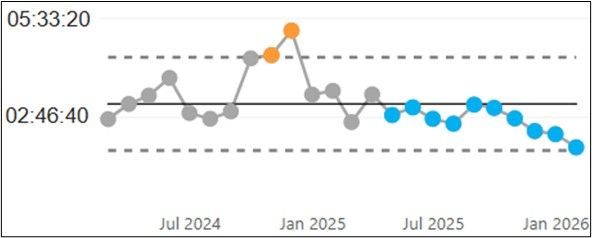
Category 3 performance July 2024 - January 2026
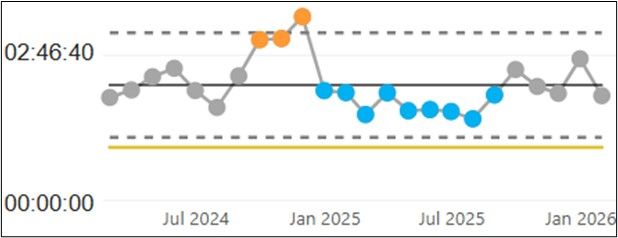
Graph summary: Line chart showing time performance from July 2024 to January 2026 with a central target line and dashed upper and lower limits. Most 2024 values (grey) sit near the target. Three late 2024 to early 2025 points (orange) rise above the upper limit, peaking at about 2 hours 46 minutes. Several early to mid 2025 points (blue) fall below the lower limit before returning closer to the target by late 2025.
Category 4 performance July 2024 - January 2026
Graph summary: Line chart showing time performance from July 2024 to January 2026 with a central target line and dashed upper and lower limits. Values in 2024 (grey) fluctuate around the target. Two late 2024 points and one early 2025 point (orange) exceed the upper limit, peaking at about 5 hours 33 minutes. From early 2025 onward, several values (blue) fall below the target and trend downward toward the lower limit by early 2026.
Across the year May 2025, June 2025 and March 2026 delivered the fastest C1 response times, while October, November and January recorded the slowest. For C2 response times performance was strongest in May 2025, August 2025 and March 2026 with slower response times again seen in October, November and January. These months of reduced performance align with seasonal pressures, driven by higher demand and wider system challenges.
Although improvements were seen within the year, the Trust recognises that it needs to do more to respond to patients more quickly. Reducing avoidable harm related to delays remains a key priority and is being addressed through system partnership working, operational improvement and continued clinical oversight.
Published further information for all ambulance services can be found here: www.england.nhs.uk/statistics and more detailed information relating to EEAST can be found within our Annual Report.
Hear and Treat
Not all 999 calls require an ambulance response. To ensure that emergency resources are available for those who need them most a dedicated team of Clinicians further assess appropriate 999 calls. They can provide expert advice and determine the most appropriate care pathway which may include self-care advice, referral to community or primary care services such as GP or Pharmacist or confirming that an ambulance response is required. This is known as Hear and Treat (H&T) where the focus is on ensuring patients receive the right care first time and safeguarding ambulance availability for patients who need urgent and lifesaving care.
Hear and Treat (H&T) activity demonstrated a steady increase throughout the year. Our EOC and UCCH clinicians handled 159,236 H&T cases, achieving an overall H&T rate of 16.22%.
After relatively stable performance in the first quarter of the year, we saw a clear upward trajectory from late summer onwards as shown in the chart below. Monthly H&T cases rose from 11,053 in April to a peak of 16,425 in December. This increased activity saw improvements in the H&T rate, which climbed from 14.47% in April to 18.30% in January, before stabilising at around 17-18% through the final months of the year.
Norfolk and Waveney achieved the highest H&T rate at 18.7% with Bedfordshire and Luton at 17.7%. Cambridgeshire and Peterborough had the lowest at 13.9% with Hertfordshire and West Essex at 15.4%.
The improvements noted were delivered through the Operational Productivity workstream, with a focus on supporting increased activity through enhanced clinical validation and H&T. These improvements strengthen our commitment to providing expert advice and determining the most appropriate care pathway, ensuring patients receive the right care first time while reducing unnecessary ambulance deployments.
Hear and Treat Activity
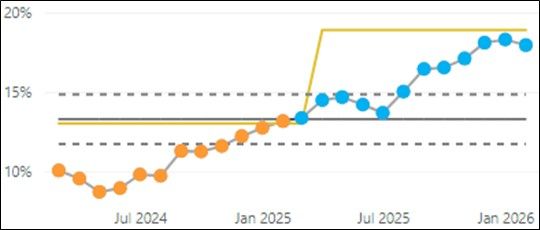
Graph summary: Line chart showing percentage performance from July 2024 to January 2026 with a central target line around 13% and dashed upper and lower limits. Values in 2024 (orange) start near 10%, dip slightly, then rise toward the target by early 2025. From early 2025, values (blue) increase above the target and trend upward, reaching around 18–19% by early 2026, with a higher target threshold line also stepping up to approximately 20%.
Operational Productivity
Across the year EEAST has focused on several operational productivity improvement measures which support delivery of the four Trust missions and ensure timely, safe and effective patient care while making the best possible use of our operational resources. These key workstreams highlight where time, capacity and workforce effort are being consumed across the whole patient journey as well as where targeted action can have the greatest impact on supporting frontline availability and service delivery.
A focused approach to this work has helped to protect response times for the most critical patients and supports a reduction in the operational pressures and strengthens wider system resilience.
The Operational Productivity measures for 2025/26 are:
- Out of service time
- On scene time (conveyed)
- On scene time (non-conveyed)
- Average hospital handover time
- Handover to clear
- Conveyance rate
- Hear & Treat
- Resource per incident
- Sickness absence
These measures support improvement by focusing attention on the points in the system where time, capacity and clinical decisions have the biggest impact on outcomes. They are designed to turn existing and funded capacity into real, usable response time for patients.
Improving our productivity measures such as reducing out-of-service time and delayed hospital handovers releases hours back into the operational day. This directly improves resource availability and protects response times for the sickest patients. When vehicles return to availability, patients receive faster response times, and the service is better able to cope with peaks in demand.
Improving conveyance and alternative pathways through hear-and-treat ensures patients receive the right care, first time. Fewer unnecessary conveyances mean less pressure on emergency departments, quicker resolution for patients, and more emergency capacity for those who need it. This improves patient experience navigating them to the most appropriate pathway for care while supporting overall system flow and service delivery.
Managing resources per incident strengthens operational resilience ensuring responses are proportionate and clinically appropriate. This reduces duplication, improves consistency and allows demand to be absorbed more effectively without compromising safety.
Reducing sickness absence supports the Trust’s financial position by making sure staff pay is spent on productive frontline hours. When fewer staff are off sick, there is less reliance on overtime or additional cover, which helps keep pay costs under control. This means the service gets more value from its existing workforce, with capacity focused on delivering care rather than funding backfill. Over time, a healthier workforce supports both financial sustainability and consistent operational performance. Overall, these productivity measures directly support the Trust’s four missions and ensuring EEAST remains responsive, resilient and focused on delivering timely, high quality care for the communities it serves.
Heart attack care
Coronary heart disease (CHD) is the most common form of heart disease and the leading cause of heart attacks and premature death in the UK. Around 100,000 hospital admissions each year are due to heart attacks. Early pre hospital identification of ST elevation myocardial infarction (STEMI), supported by timely assessment and delivery of an evidence based care bundle, significantly improves patient outcomes. This approach reduces mortality, supports faster recovery, and aligns with NHS priorities to prevent avoidable deaths and improve recovery following acute illness.
STEMI care bundle
The mandatory ambulance services quality indicator for STEMI relates to the delivery of an appropriate care bundle, including the recording of two pain scores, administration of aspirin, and provision of pain relief. Patient care records are audited against these criteria and classified as compliant or non-compliant. Performance is reported quarterly.
The table below presents the Trust’s compliance compared with the national average and the best and worst performance achieved by ambulance services in England. Data published to date (April–October 2025) demonstrate that the Trust’s performance is consistently above the national average for each quarter, as illustrated in the accompanying graph.
National data (April - October 2025)
| Heart attack care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| STEMI Care Bundle | 82.6% | 95.9% | 73.5% | 95.9% |
EEAST was the highest performing ambulance trust for this time period, averaging 13.3% above the national average.
ACQI STEMI Care Bundle performance from January 2025 to January 2026
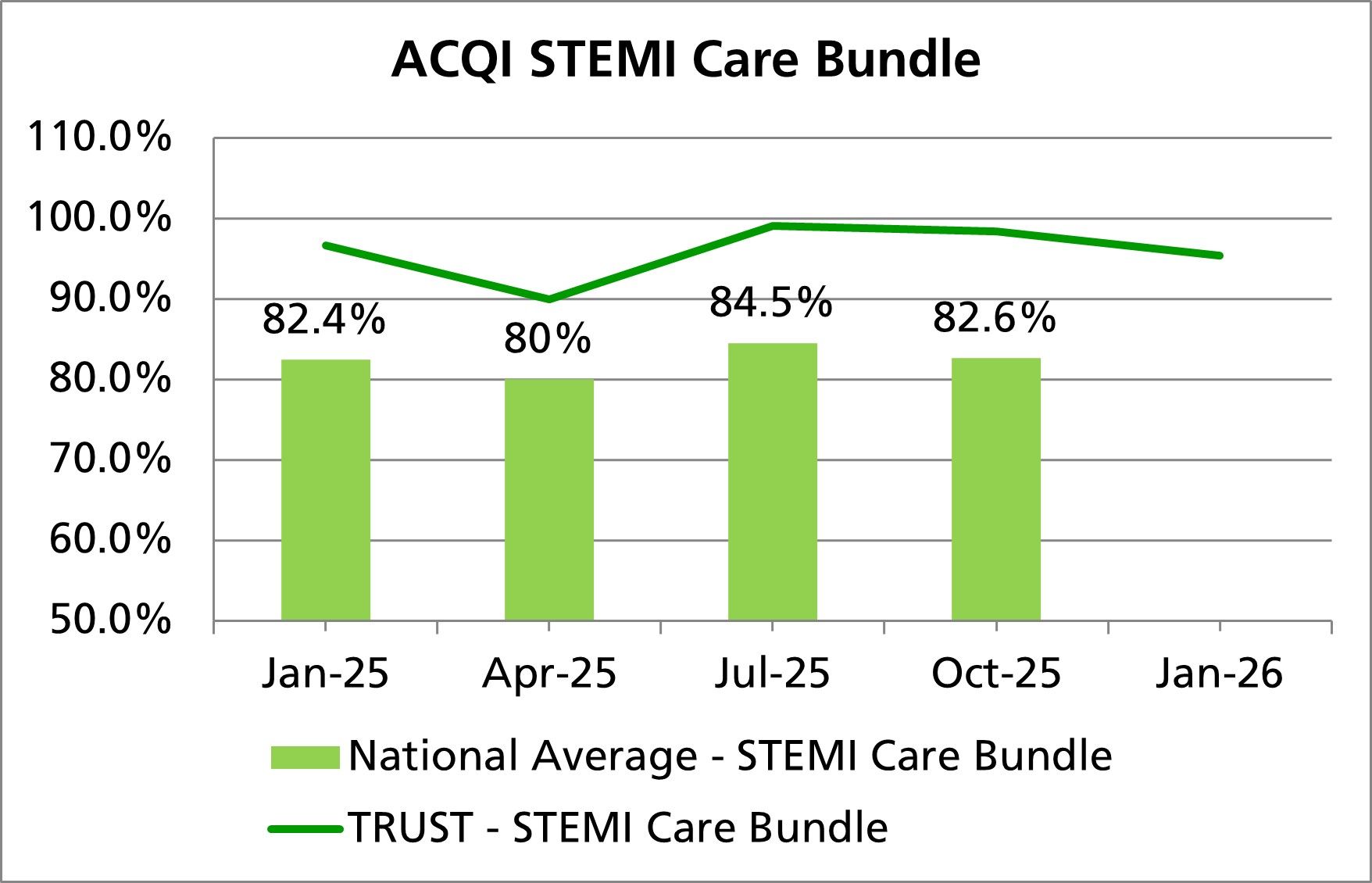
Graph summary: National average (bars) is 82.4% in January 2025, drops to 80% in April, rises to 84.5% in July, and is 82.6% in October. Trust performance (line) is higher throughout, dipping around April before peaking near 99% in July and then slightly declining to the mid 90s by January 2026.
Patients conveyed to a Primary Percutaneous Coronary Intervention (PPCI) Centre
Although transport time to a specialist Primary Percutaneous Coronary Intervention (PPCI) centre is not a formal Quality Account metric, performance is monitored and reported monthly to NHS England and commissioners. The Ambulance Clinical Quality Indicator (ACQI) comprises two joint time-based indicators for ambulance trusts and PPCI centres, measured in hours and minutes.
The table below presents the Trust’s performance compared with the national average and the upper and lower performance levels achieved by ambulance services in England for published data (April–October 2025). It should be noted that the lower value represents the best performance outcome for these measures.
Latest data available April – October 2025 hh:mm
| Heart attack care | National average | Upper | Lower | EEAST Performance |
|---|---|---|---|---|
| Mean average time from call to catheter insertion for angiography | 02:26 | 02:33 | 02:13 | 02:33 |
| 90th centile time from call to catheter insertion for angiography | 03:16 | 03:29 | 02:54 | 03:21 |
As shown in the table above, EEAST performed outside of the national average for both of these measures, but, as demonstrated in the previous section, all patients received excellent care, with EEAST consistently achieving high compliance for the STEMI care bundle and being the highest performing trust within the year.
Next steps: As well as continually being monitored through the national ACQI programme, one of the Trust’s ongoing priorities is to reduce our response times to Category 2 calls which include STEMI patients.
Stroke care - timeliness
Patients who receive care in a dedicated stroke unit with organised stroke services are more likely to survive, experience fewer complications, and return home sooner with greater levels of independence than those treated on a general medical ward. Timely access to specialist stroke care is therefore a key component of the Trust’s commitment to delivering safe, effective and high-quality care.
Although the time taken to convey a suspected stroke patient to hospital is not a mandated quality metric within the NHS England Quality Account framework, the Trust monitors and reports this measure on a month-by-month basis to NHS England and its commissioners as part of its wider clinical quality assurance arrangements. This provides additional assurance regarding system performance and supports continuous improvement in urgent and emergency care pathways. Performance for this Ambulance Clinical Quality Indicator (ACQI) is assessed monthly against three nationally recognised measures: mean average, median, and 90th centile times from receipt of the emergency call to arrival at hospital. Monitoring these indicators enables the Trust to identify variation in performance, understand the experience of patients with the longest waits, and take targeted action where required.
The table below presents the Trust’s performance in comparison with the national average, together with the upper and lower performance levels achieved by ambulance services across England, using data published between April and October 2025. The lower level represents the best-performing trust nationally for this outcome.
In interpreting this data, it is important to recognise known limitations. Not all strokes are identified at the point of the initial emergency call, as this depends on the information available to the call handler at that time. In addition, some patients may deteriorate either before the ambulance crew arrives or after they are on scene, which may affect conveyance times. These factors are routinely considered as part of internal performance review and quality assurance processes.
National data – April to October 2025 hh:mm
| Stroke care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| Mean average time from call to hospital arrival | 01:30 | 01:43 | 01:18 | 01:30 |
| Median time from call to hospital arrival | 01:19 | 01:31 | 01:10 | 01:20 |
| 90th centile time from call to hospital arrival | 02:16 | 02:38 | 01:58 | 02:19 |
On average EEAST performed just outside the national average for two of the three indicators for this period.
Next steps: This will continue to be monitored through the national ACQI programme. One of the Trust’s continuing priorities is to reduce our response times to Category 2 calls which includes stroke patients.
Cardiac arrest care
Cardiac arrest occurs when the heart suddenly stops pumping blood around the body. A person experiencing a cardiac arrest will abruptly lose consciousness and may stop breathing or breathe abnormally. Without immediate treatment, cardiac arrest is fatal within minutes. Early intervention through high-quality cardiopulmonary resuscitation (CPR) and prompt defibrillation can, however, significantly improve the chances of survival and recovery.
Approximately two-thirds of out-of-hospital cardiac arrests occur in the home. In contrast, nearly half of cardiac arrests occurring in public places are witnessed by bystanders, highlighting the critical importance of public awareness and rapid response. For every minute that passes without defibrillation following cardiac arrest, the likelihood of survival decreases by approximately 10%.
Although the indicators are not designated quality metrics within the Quality Account, performance against these measures is routinely monitored and reported to NHS England and local commissioners monthly, except for the Post-Return of Spontaneous Circulation (ROSC) care bundle, which is reported on a quarterly basis.
The Post-ROSC care bundle comprises of six elements that must be recorded and administered to all patients who achieve ROSC on scene and are subsequently conveyed to hospital. These include:
- 12-lead electrocardiogram (ECG)
- Measurement of blood glucose
- Monitoring of end-tidal carbon dioxide (EtCO2)
- Administration of appropriate oxygen therapy
- Measurement and management of systolic blood pressure
- Administration of intravenous saline fluids
The table below presents our performance against the national average, together with the highest and lowest levels achieved by ambulance services in England, based on published data covering the period from April to October 2025.
National data – April – October 2025
| Cardiac arrest care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| Return of Spontaneous Circulation (pulse) at hospital – All patients | 28.4% | 31.6% | 18.9% | 31.6% |
| Return of Spontaneous Circulation (pulse) at hospital – Utstein patients | 50.9% | 63.6% | 44.2% | 52.8% |
| Survival to Discharge – All patients | 10.2% | 12.2% | 6.8% | 11.3% |
| Survival to discharge – Utstein patients | 30.5% | 38.0% | 25.0% | 31.9% |
| Post-ROSC care bundle | 80.7% | 95.8% | 53.9% | 95.8% |
EEAST performed higher than the national average and was the highest performing trust for achieving ROSC (all patients group) and Post-ROSC care bundle. It was also the third highest for the remaining indicators for these patients It should be noted that not all ambulance trusts submitted full data, so these outcomes. It was also the third highest for the remaining indicators for these patients It should be noted that not all ambulance trusts submitted full data, so these outcomes.
Next steps: This will continue to be monitored through the national ACQI programme. Successful outcomes from cardiac arrests are, in part, due to actions taken by acute organisations following arrival at hospital as well as early access to treatment and intervention.
Patient safety incidents
A patient safety incident is defined as any unintended or unexpected incident which could have or did lead to harm for one or more patients receiving NHS care. This includes:
- incidents that caused no harm or minimal harm,
- incidents with a more serious outcome,
- prevented patient safety incidents (known as ‘near misses’).
The number of incidents reported by staff during 2025/26 demonstrates a good culture of reporting and being open and honest, incident reporting remains stable across the organisation in comparison to previous years. Where a near miss has happened, proactive steps can be taken to reduce the risk going forwards and to maintain a learning from incidents culture. The overall number of patient safety incidents relating to delays has decreased as illustrated in the chart below. The charts below demonstrate our performance for both of these points.
Incidents from February 2024 to February 2026
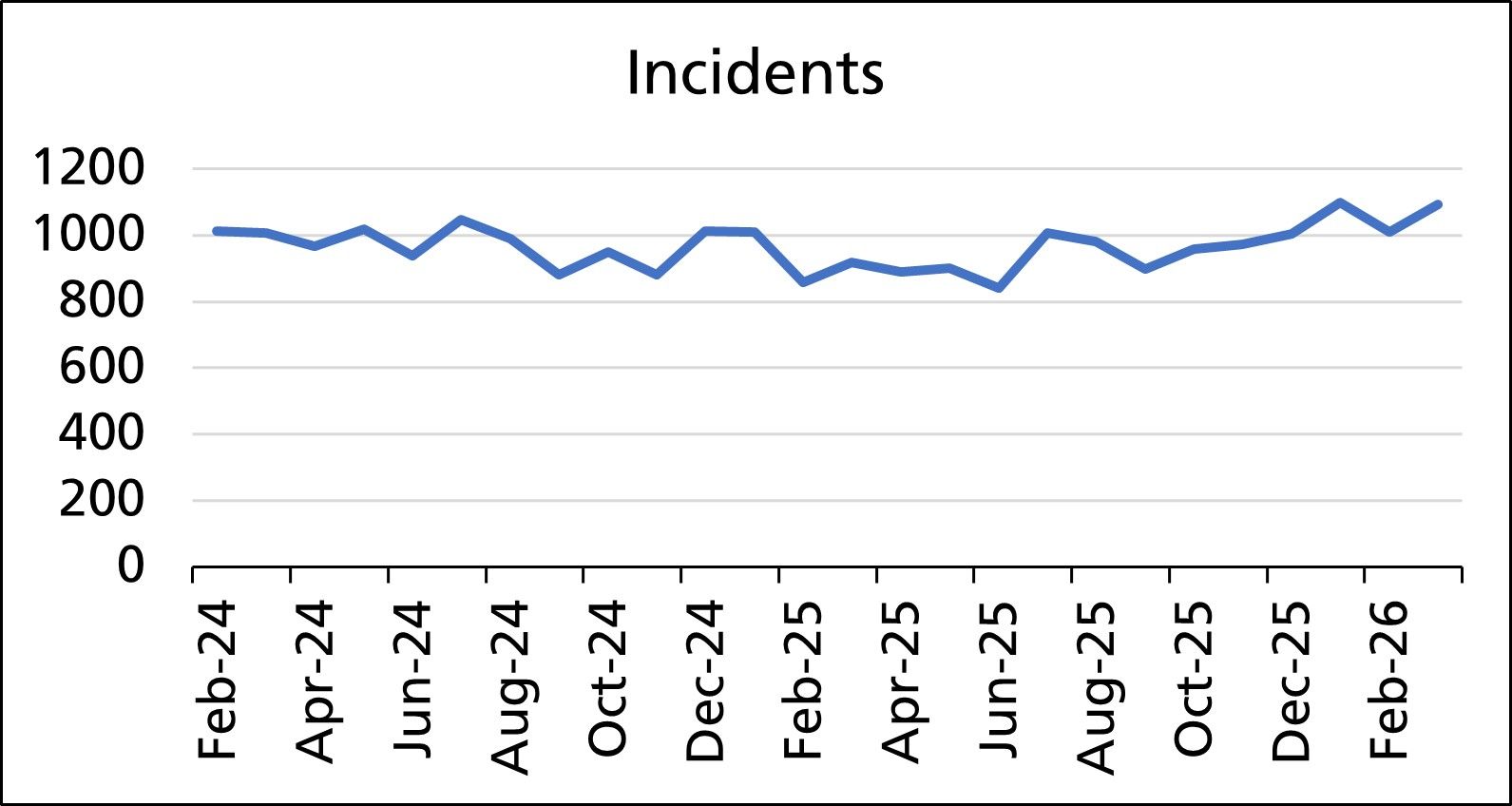
Graph summary: Values fluctuate between approximately 850 and 1,100 incidents, with several peaks around mid 2024, late 2025, and early 2026, and dips in early and mid 2025. Overall, the trend remains relatively stable with minor variation over time.
Patient Safety Incidents and UEC Delays from April 2024 to March 2026
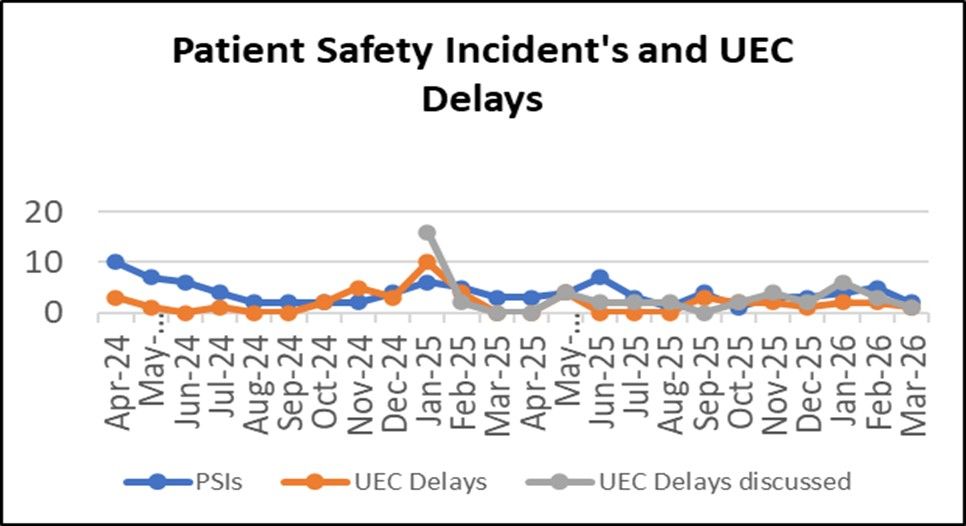
Graph summary: Three series are displayed: PSIs (blue), UEC delays (orange), and UEC delays discussed (grey). PSIs fluctuate between around 2 and 10 incidents, with a peak in mid 2025. UEC delays remain low, mostly between 0 and 5, with a brief rise in late 2024. UEC delays discussed show a notable spike above 15 in early 2025 before returning to lower levels. Overall, values across all three measures vary but remain relatively low.
Prior to the implementation of the Patient Safety Incident Response Framework (PSIRF) EEAST reported on the level of harm they directly caused in relation to individual incidents. Since the implementation of PSIRF in October 2024, the parameters to which levels of harm are reported have been updated in line with Learning from Patient Safety Events (LFPSE) guidance to reflect how EEAST may have contributed towards harm. A condition within the Quality Account requirements is for each trust to provide a comparison of their patient safety incidents reported to NRLS against the national average for similar services, however, this process is no longer available.
Patient experience and feedback
As a Trust, we are committed to demonstrating how we continually develop and improve our services based on the experiences and feedback of the people who use them. Patients, families and our wider communities are central to everything we do and their voices play a vital role in shaping and driving service improvement.
The following pages outline what patients and families have told us through public engagement, complaints, compliments and surveys, the actions we have taken in response and how we plan to improve further. This reflects our commitment to learning, transparency and working in partnership with people and communities.
The Patient Experience Department leads and co-ordinates complaints, compliments and patient and public engagement activity. Our approach aligns with the NHS Complaints Regulations 2009, the Parliamentary and Health Service Ombudsman (PHSO) Framework, NHS England’s Experience of Care Framework (2025) and the statutory guidance on Working in Partnership with People and Communities (2022), as well as local policy.
All feedback, whether positive or negative, is recorded and managed by the department. We ensure ongoing communication with patients and families throughout the process, and provide clear, timely responses to their feedback. Our focus is to resolve concerns wherever possible, ensuring complaints are handled compassionately and fairly, whilst identifying opportunities for learning and improvement.
Compliments
Compliments continue to significantly exceed the number of complaints received. In 2025/26, the Trust recorded 3,722 compliments, an average of 310 per month. This equates to a compliment to complaints ratio of 6:1, evidencing continued positive patient experience.
Compliments are reported to the Trust Board, communicated directly to colleagues involved, and added to the staff member’s personnel file. Over the past year, the main themes arising from compliments have related to the professionalism, kindness and care demonstrated by Trust staff. By adopting an Appreciative Inquiry approach, the Trust uses learning from excellence to reinforce positive behaviours and support the delivery of effective, compassionate care across the organisation.
| Apr-25 | May-25 | Jun-25 | Jul-25 | Aug-25 | Sep-25 | Oct-25 | Nov-25 | Dec-25 | Jan-26 | Feb-26 | Mar-26 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Compliment | 314 | 279 | 249 | 293 | 322 | 304 | 384 | 254 | 318 | 372 | 337 | 296 |
| Complaint | 65 | 70 | 59 | 42 | 46 | 62 | 46 | 54 | 53 | 48 | 47 | 57 |
Complaints
In 2024/25, the Trust changed its approach to categorising expressions of dissatisfaction, with concerns and complaints no longer recorded separately. All expressions of dissatisfaction are now reported as complaints. This approach has continued in 2025/26 and supports greater consistency, transparency and alignment with the Parliamentary and Health Service Ombudsman (PHSO) Complaints Standards Framework.
During 2025/26, 649 complaints were received, representing a reduction from 868 complaints in 2024/25. Complaint volumes have remained low and stable, reflecting sustained improvement following earlier periods of higher activity.
Complaints accounted for 0.04% (649/1,490,823) of all patient contacts in 2025/26, compared with 0.05% in 2024/25. Where complaints cannot be resolved through early resolution, they progress to a local investigation and may also be reviewed by the Patient Safety Team where appropriate. Unfortunately, no benchmarking data for complaints by patient contact relating to ambulance services is currently available.
An anonymised sample of complaint responses was reviewed earlier in the year by Community Engagement Group (CEG) volunteers, who acted as ‘critical friends’ and provided feedback to support improvements in response quality. This activity has been temporarily paused due to departmental capacity, with plans to resume in 2026/27.
In total, 28 complaints (4.3%) were re-opened during the year. While overall complaint numbers remain low, this represents an increase compared with 2024/25. Re-opened cases will be reviewed to identify learning and inform further improvements to complaint handling and response quality.
Re-opened complaints 2025/26 (April 2025 to March 2026)
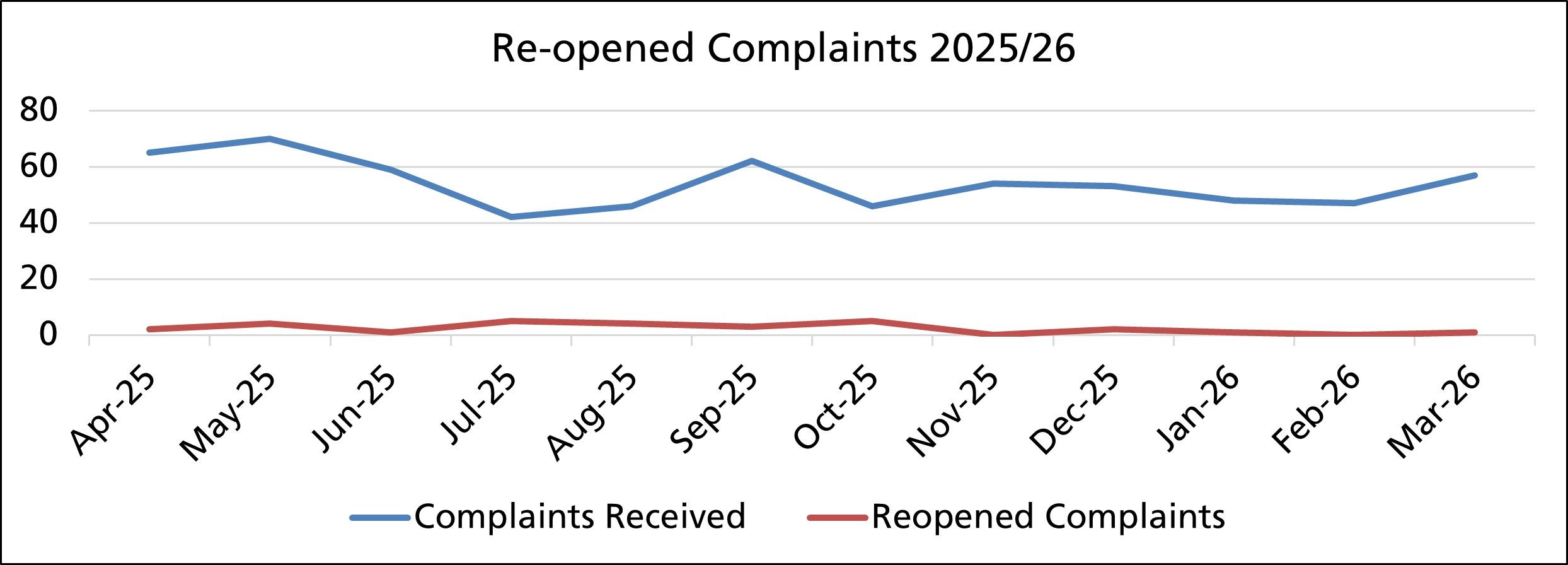
Graph showing the number of compliments and complaints received each month during the year.
Graph summary: Complaints received (blue line) fluctuate between around 40 and 70, peaking in May and September and dipping in July. Reopened complaints (red line) remain consistently low, ranging from 0 to about 5, with small increases in July and October. Overall, complaint volumes vary moderately while reopened cases stay minimal.
Complaint Themes
Emergency and Urgent Care (EUC)
Complaint themes within Emergency and Urgent Care (EUC) have remained broadly consistent with 2024/25. Complaints continue to relate primarily to clinical assessment and treatment, and staff attitude. Within the Emergency Operations Centre, complaints mainly focus on delays, communication and call handling.
Despite sustained winter pressures under REAP 4, complaints relating to delays have remained relatively low during the winter period.
Misunderstanding about triage processes and emergency call prioritisation remains a recurring theme. This reinforces the continued importance of clear and effective communication with patients and callers, particularly as the Trust implements its Patient Plan to support delivery of the right care, at the right time, by the right person.
Patient Transport Service (PTS)
As in 2024/25, dissatisfaction within Patient Transport Services (PTS) continued to relate primarily to delays and transport or driving related issues. Communication remained a significant contributing factor, particularly where transport was delayed or did not attend, with some complaints also reflecting uncertainty or misunderstanding regarding vehicle suitability or equipment requirements.
While complaint themes remained broadly consistent across service lines, there was clear evidence of improvement, reflected in a sustained reduction in overall complaint volumes during 2025/26. Significant reductions were observed across several key themes, including delays (34% reduction), staff attitude (30% reduction), clinical treatment and assessment (14% reduction), transport and driving (43% reduction), and communication and call handling (29% reduction).
These reductions reflect the positive impact of targeted improvement activity across the Trust. Within Emergency and Urgent Care (EUC), the reduction in delay related complaints aligns with the Trust’s delay action plan and the implementation of the 45 minute handover process in partnership with acute hospital providers. The reduction in complaints relating to clinical treatment and assessment may also reflect the continued embedding of the Trust’s clinical model, supporting improved clinical decision making and more appropriate patient pathways.
Within PTS, improvements to booking processes, clearer journey prioritisation and a reduction in the number of contracted providers have contributed to fewer delay and transport related complaints. Further developments in planning and scheduling arrangements have also reduced concerns related to transport and driving reliability. Overall, the sustained reduction in complaints relating to staff attitude and communication provides assurance of the positive impact of the Trust’s continued focus on culture, behaviours and compassionate communication. This work is delivering measurable improvements in patient experience and remains a key area of ongoing focus within the Trust’s quality improvement programme.
Parliamentary and Health Service Ombudsman (PHSO)
Although the majority of complaints are resolved through the Trust’s local complaints process, complainants may refer their concerns to the Parliamentary and Health Service Ombudsman (PHSO) for an independent review where they remain dissatisfied and all stages of the Trust’s process have been exhausted. The PHSO provides an impartial assessment of complaints and offers independent recommendations to support learning and improvement in complaint handling, investigation quality and organisational practice.
During 2025/26, the Trust was notified of one complaint referred to the PHSO. There are no historic complaints outstanding and no cases currently under review by the PHSO.
You said, we did
As a Trust we recognise the importance of learning when things have not gone as well as we would have liked or from our patient survey feedback. The following case studies are just three examples of some of the learning from last year.
| You said | What we did | What this means |
|---|---|---|
| Patient feedback from the Stroke Video Triage survey often highlighted difficulties with poor mobile signal, which affected video quality and connection stability. Feedback also related to the limited availability of the Stroke Video Triage Service across the region, meaning some patients were unable to access the pathway depending on where they lived or when triage was needed. | We initiated a trial with Excelerate, fitting ambulances with on board WiFi to improve connection stability during video assessments and in known poor signal areas. We have expanded Stroke Video Triage availability across the region. The pathway is now active at 12 of the 15 Stroke Centres in the East of England, including: 24/7 access at six centres. Extended hours, 7 day a week service at four centres. Expansion planned for the remaining two centres from April 2026, supporting full regional coverage. | The on board Wi Fi trial has significantly reduced connection issues, allowing for a more reliable and consistent video link, even in areas with poor network coverage or while the vehicle is moving. Increased availability means more patients can now benefit from rapid specialist triage, reducing unnecessary hospital conveyance and supporting faster onward referral to TIA and stroke services. The expansion positions the region to achieve full 24/7 stroke triage access across all 15 centres, improving equity of access and ensuring patients receive timely specialist assessment regardless of location or time of day. |
| Younger patients (16 to 24) have historically reported lower satisfaction with the service compared with other age groups. Young people aged 16 to 17 were previously unable to join the Community Engagement Group (CEG), limiting representation of their views. Feedback also highlighted the need for better engagement with children and young people, including more accessible ways to share their experiences. | We have introduced new policies and processes enabling 16 to 17 year olds to volunteer safely as CEG members, improving representation of younger voices. Additionally, we have recruited the first young member aged 16 to 24, with two additional young people currently onboarding. This is supported by strengthened induction processes for those under 18. Engagement with young people is now one of the CEG’s three key priorities, with an established dedicated working group involving members under 25 years old. The working group is actively exploring why younger patients report lower satisfaction. We have expanded engagement activity, including work experience, school and college visits and careers fairs. | EEAST now has structures in place to embed young people’s voices in service improvement, helping ensure their experiences directly influence decision making. Early signs show improvement: in 2025/26, 87.1% of 16 to 24 year olds rated their overall satisfaction as good or very good, which compares with 75.0% in 2024/25. Though numbers remain small and should be interpreted with caution. Continued work through the CEG and the new youth engagement working group will help build a better understanding of this age group’s needs, ensuring services and communication are more accessible and relevant to them. |
| Maternity patients have told us that they can feel vulnerable and exposed when multiple crew members remain in the room during intimate assessments. | This feedback has been incorporated into frontline maternity teaching. Crews are reminded that, once the initial assessment is completed, only essential crew members should remain, with non-essential crew waiting elsewhere to maintain privacy, dignity and comfort. | Maternity patients will now experience greater dignity and privacy during intimate assessments. This approach will create a calmer and more respectful environment, reduce feelings of vulnerability, and reinforce our commitment to delivering care that is sensitive, person centred and aligned with best practice. |
Patient surveys
The Trust undertakes a comprehensive annual patient survey programme, which includes continuous surveys for the urgent and emergency care service (UEC) and the patient transport service (PTS).
Patient surveys are promoted using a variety of methods, including the Trust’s social media channels, invitation to feedback letters and patient information cards. During 2025/26, 63.0% of PTS survey submissions were generated directly through SMS signposting.
Listening to the patient voice enables the Trust to understand what is working well and to identify areas requiring improvement. Feedback from surveys is routinely monitored and triangulated with themes from complaints, patient engagement activity and patient safety data to ensure robust governance, shared learning and continuous improvement in patient experience and outcomes. This approach enables the Trust to recognise areas of excellence and embed positive practice across services provided by EEAST.
All patient surveys include the Friends and Family Test (FFT) question, ‘Overall, how was your experience of our service?’ The FFT provides a benchmark of overall satisfaction across the Trust. The score is calculated by dividing the proportion of ‘very good’ and ‘good’ responses by the total number of responses.
The FFT is a national directive, and the Trust is required to provide all PTS patients with the opportunity to respond to the FFT question, with results reported monthly to NHS England.
FFT results from 2024/25 and 2025/26 can be found below. The 2025/26 survey results show higher overall patient satisfaction and increased response numbers across the Trust, with notable improvement in UEC and consistently high, stable satisfaction in the PTS.
Overall Satisfaction (Friends and Family Test)
| Continuous Patient Survey Results: | Number of patients: 2024/25 | Overall Satisfaction: 2024/25 | Number of patients: 2025/26 | Overall satisfaction: 2025/26 |
|---|---|---|---|---|
| Urgent and Emergency Care | 702 / 815 | 86.1% | 898 / 991 | 90.6% |
| Patient Transport Service | 1612 / 1865 | 86.4% | 2401 / 2087 | 86.9% |
| All Services | 2314 / 2680 | 86.3% | 3078/3299 | 93.3% |
Survey projects
This section provides further information on each of the surveys undertaken throughout the year.
Easy Read
The easy read survey, co-produced with the D.R.A.G.O.N.S at the Norfolk and Norwich SEND Association (NANSA), continues to be available as an accessible feedback option for UEC and PTS patients. This survey option enables people to share their experiences in a meaningful way and ensures feedback contributes directly to learning, improvement and informed decision making.
Feedback received during 2025/26 has been largely positive about the service and staff (FFT score: 93.7%). Patients reported feeling listened to and noted that staff communicated clearly and supported any individual sensory needs. The main area of dissatisfaction has related to ambulance and PTS delays; with this feedback shared as part of the wider system review.
This survey continues to highlight the value of co-production and working in equal partnership with experts by experience. The co-production work undertaken with the NANSA D.R.A.G.O.N.S group in 2024/25 resulted in the development of an accessible explanatory video to support patients in completing the easy read survey and understanding how their feedback is used. While the development work was concluded last year, this resource remains available and continues to play an important role in supporting patients to engage with the survey and understand how their feedback will inform service improvement.
Maternity
The maternity survey has continued as an online feedback option during 2025/26, enabling patients to share their experiences following a maternity related 999 emergency call.
Patients have continued to report a positive experience of staff and the service provided (95.8%), with areas of dissatisfaction generally relating to communication/attitude and ambulance delays. Feedback received has also highlighted that patients can feel vulnerable when multiple people are present in a room during intimate assessments. This feedback has been shared with the Clinical Lead and Clinical Specialist Midwife, and the learning has been incorporated into teaching for frontline crews. Crews are now advised that, following the initial assessment, non essential crew members should wait elsewhere in the property to support patient dignity, privacy and comfort.
Stroke video triage
Over the past year, the stroke video triage survey continued to proactively gather feedback from patients receiving a pre hospital video assessment, supporting timely and appropriate care. The pathway has improved arrival to imaging times and reduced treatment delays across all live centres.
Patient satisfaction remains high (80%), but qualitative feedback has indicated that many patients or relatives were unaware that a stroke video assessment had taken place. In response, communication has been strengthened so that crews clearly explain when and how a video assessment is being conducted. Surveys are also now sent out closer to the time of the incident, helping to increase response rates and gather clearer, more detailed feedback from patients and relatives
Patient feedback has directly shaped service improvements over the past year. Reports of poor mobile signal has led to fitting ambulances with on board Wi Fi, which has significantly reduced connection issues. Feedback relating to the limited operating hours has informed the expansion of Stroke Video Triage across the region – which is now available at 12 of 15 Stroke Centres, with increasing 24/7 and extended hours coverage and plans for full 24/7 access across all centres.
Survey findings have been shared widely with NHS England, the Integrated Stroke Delivery Network, national and international conferences and ongoing research projects, helping to raise the profile of EEAST and demonstrate the pathway’s impact on patient experience, outcomes, and optimisation of the pre hospital stroke pathway.
Mental health
During 2025/26, a new Mental Health Response Vehicle (MHRV) survey was co produced with the Clinical Lead for Mental Health, mental health practitioners, commissioners and Experts by Experience to support system wide learning and improvement for patients in mental health crisis.
The survey gathers feedback from patients attended by the MHRV and helps evaluate how effectively the service supports people in mental health crisis, including whether specialist assessment is provided in a timely and appropriate way.
Following contact with the MHRV, patients are given a leaflet that explains the MHRV model, provides signposting, offers a practical action plan for patients, supporters and carers and includes an opportunity to give valuable feedback via an online survey. Insights from the survey are used to evidence satisfaction, outcomes and impact, and to inform service refinement and the case for longer term funding and wider implementation.
Although feedback gathered so far is limited due to the early stage of the initiative, responses received to date remain highly positive, with 100.0% satisfaction reported from eight MHRV survey respondents. A separate online mental health survey received two responses, both raising concerns about communication and perceived lack of mental health support; these have been shared with the Clinical Lead for Mental Health and the Mental Health Advanced Practitioner to support wider learning.
Although MHRV feedback is very positive, broader feedback from the online survey and other sources continues to indicate a need for stronger mental health support and clearer signposting.
Admission avoidance
Several admission avoidance surveys have continued during 2025/26 in support of the clinical model. These surveys capture feedback from patients treated safely at home, many of whom avoided need for hospital conveyance. Feedback across the Physician Response Unit, Advanced Practice Team and Community Wellbeing teams has been overwhelmingly positive, with high satisfaction reported (100.0% for the Physician Response Unit and Community Wellbeing Officer, and 96.0% for the Advanced Practice Team).
Where concerns were raised, these have largely related to delays or communication. Survey feedback also indicates that patients are not always aware of the full range of services or the potential outcomes following 999 emergency call triage. This reinforces the need for clearer communication about the clinical model (Patient Plan) and alternative pathways in place.
Patient feedback continues to provide essential evidence of satisfaction and outcomes, helping to refine services and support the case for sustained funding and region wide implementation. Engagement activity during 2026/27 will focus on improving public understanding of the Patient Plan and increasing awareness of pathways available.
A Patient Voice Task and Finish Group has co produced a Patient Voice Framework, providing a consistent approach to embedding lived experiences and ensuring the patient voice is at the heart of service design and evaluation. The framework will be introduced using a phased approach and initially tested via the Patient Plan and health inequalities work. As it embeds, reporting is expected to show greater awareness of the Patient Plan and stronger, more meaningful patient feedback.
Next steps
In 2026/27, we will continue to strengthen how patient and community feedback shapes improvement across the Trust. Key priorities include:
- Implementing the co-produced Patient Voice Framework, which will initially be trialled via the Patient Plan and health inequalities work.
- Ongoing engagement activities will focus on supporting the Patient Plan and helping patients and the public understand the different pathways available.
- Strengthening complaints learning, including resuming CEG complaint reviews, improving first time resolution and ensuring clearer, more compassionate responses.
- Continuing targeted recruitment to the CEG to improve diversity and regional representation across the region.
- Supporting CEG working groups to progress their priority areas, including youth engagement, walkabout audits and bystander support initiatives.
- Expanding accessible feedback routes, including further digital options and co produced formats to widen participation.
- Continuing a prioritised patient survey programme focused on learning and improvement, aligned with Trust priorities.
- Ongoing admission avoidance feedback projects, alongside development of a new unscheduled care hub survey with system partners.
- Supporting pathway improvements, including full 24/7 Stroke Video Triage coverage, further development of the MHRV model, and the out of hospital video guided CPR initiative.
These actions will ensure the patient voice continues to drive meaningful improvement in the safety, quality and responsiveness of care across EEAST.
