Annual Quality Account 2024-2025
Date published: 25 June 2025
Summary
Welcome to the East of England Ambulance Service NHS Trust Quality Account for 2024/25. This document has been approved by the Trust Board and is an accurate account of the level of quality of service provided to patients. In developing this Quality Account, we have set out a summary of achievements for 2024/25 and goals for 2025/26 as mandated within the regulatory guidance.
In this report
- Part One
- Foreword and statement on quality from the Board
- Welcome to the East of England Service NHS Trust (EEAST) Quality Account
- Introducing the East of England Ambulance Service NHS Trust Quality Account and Improvements
- What is a Quality Account and what does it mean to EEAST and the people we serve?
- Our current quality position
- Care Quality Commission
- Department of Health Core Quality Indicators
- NHS Number and General Medical Practice code validity
- NHS clinical coding error rate
- Data quality
- Data security protection toolkit
- Statement of Accountability
- Part Two:
- Quality improvement initiatives
- Priority one: Patient safety
- Priority Two - Clinical effectiveness
- Priority Three - Patient Experience
- Part Three
- Progress on the quality account priorities 2024/25
- Performance of the Trust against quality metrics
- Achievements against local priorities set for 2024/25
- Clinical audit
- Participation in research
- Patient Safety Incidents
- Serious Incidents
- When things go wrong
- Duty of Candour
- National Patient Safety Alerts
- Patient experience and feedback
- Patient and public involvement
- Raising concerns and Freedom to Speak Up
- Working with our local communities
- Commissioning for Quality and Innovation (CQuIN)
- Quality success throughout the year
- Quality Governance Committee Assurance
- Statements from stakeholders
- Glossary
What is a Quality Account and what does it mean to EEAST and the people we serve?
A Quality Account is a mandatory report about the quality of services an NHS healthcare trust provides and is required to be completed in line with the Health and Social Care Act 2012.
Quality reports and accounts are set against the framework of three overlapping key themes, patient safety, clinical effectiveness and patient experience, which can be used to define quality of care.
The content is defined by NHS England and includes outcome results against specific indicators under five headings:
- Preventing people from dying prematurely.
- Enhancing quality of life for people with long term conditions.
- Helping people to recover from episodes of ill health or following injury.
- Ensuring that people have a positive experience of care.
- Treating and caring for people in a safe environment and protecting them from avoidable harm.
In addition to information provided within this report, our newly published Corporate Strategy 2025/30 details what we are aiming to achieve over the next five years and how we are going to do this.
Performance of the Trust against quality metrics
Response Times
Ambulance services are monitored against response times for a Category 1 – 4 system (determined by clinical condition/emergency), with varying response times for each category. The table below summarises the Trust’s performance against the national response time standards for 2024/25.
Although not meeting the national standards, except for the C1 (7 minutes mean and 90th centile) which was six seconds longer than the previous year, all categories were improved on the previous year with the exception of the C1 (7 minutes mean) which was six seconds longer than the previous year.
| Category | Definition | National standard | Average EEAST Performance 2023/24 and 2024/25 |
|---|---|---|---|
| C1 | Immediately life-threatening injuries and illnesses. | 7 minutes mean response time | 00:09:03 and 00:09:08 |
| 15 minutes 90th centile response time | 00:17:04 and 00:17:12 | ||
| C2 | Emergency. | 18 minutes mean response time | 00:43:51 and 00:42:49 |
| 40 minutes 90th centile response time | 01:35:56 and 01:32:50 | ||
| C3 | Urgent calls and in some instances where patients may be treated in-situ (e.g., their own home) or referred to a different pathway of care. | 120 minutes (2 hours) 90th centile response time | 05:03:57 and 02:21:56 |
| C4 | Less urgent. In some instances, patients may be given advice over the phone or referred to another service such as a GP or pharmacist. | 180 minutes (3 hours) 90th centile response time | 08:49:30 and 03:54:56 |
- Category C1 calls - maintained a consistent response time, averaging around 9 minutes across all months with a total average of 00:09:08.
- Category C2 calls - showed fluctuations throughout the year, peaking at 00:57:20 in December 2024 but averaging 00:42:42.
- Category C3 calls - had response times ranging from 01:39:49 to over 3 hours, with an overall mean of 02:20:51.
- Category C4 calls - consistently had the longest response times, exceeding 3 hours in multiple months, with an overall mean of 03:33:00.
March 2025 saw the best response times for the year for all categories.
- C1: 00:08:32 C2: 00:32:47
- C3: 01:38:57 C4: 02:30:00
Published further information for all ambulance services can be found here: www.england.nhs.uk/statistics and more detailed information relating to EEAST can be found within our Annual Report.
During the year, the Trust implemented several initiatives to enhance staffing levels and workforce effectiveness:
-
Recruitment and retention efforts: EEAST has successfully reduced staff turnover through a well-planned strategy, maintaining a strong workforce with valuable experience and skills, while saving on recruitment and external staffing costs.
-
Implementation of the 'Time for Me' wellbeing platform: In May 2024, EEAST launched 'Time for Me,' a platform powered by Hapstar, to support mental health and wellbeing. With nearly 700 employees and volunteers registered, over 60,000 wellbeing data points have been captured, enabling targeted support and early intervention.
-
Adoption of the NHS Long Term workforce plan: EEAST aligns with the NHS Long Term Workforce Plan, focusing on expanding education, training and recruitment to ensure a sustainable and resilient workforce.
-
Implementation of E-rostering and effective job planning: EEAST utilises electronic rostering and effective job planning to ensure appropriate staffing levels, enhancing productivity and patient care.
Our Operational Improvement Plan contains further actions to improve our performance, these include but are not limited to;
-
Reduction of our job cycle time (JCT) – JCT represents the total time taken to assist a single patient. The shorter the time taken the more patients can potentially be assisted. The largest part of the JCT is typically the on-scene times and these are within our control. Reducing on-scene times is crucial for providing care that aligns with the standards of other UK ambulance services and ultimately benefits the patient.
-
Roll out of Organisational Information portal (OIP), This action allows the visibility of individual performance and is planned for rollout alongside a framework of performance appraisals. OIP has now been rolled out Trust wide and is monitored locally by the management teams and progress reviewed through the regular Organisational Performance Improvement Plan (OPIP) meetings.
-
Education programme on clinical best practice on scene decision making. Led by the clinical leads, this education programme is designed to support staff outside of the normal on scene time ranges. All sectors have produced plans to roll out education.
In January 2025 the Trust received a Regulation 64 notification regarding our response times to category two patients. Further information relating to this can be found within the CQC section of this report on pages 11-14.
One factor affecting our C2 performance is the number of service provision hours lost – this can be impacted by a variety of causes however the biggest impact on the ambulance service within this are delays in handing patients over at our hospitals.
A national standard of 15 minutes is in place for our staff to handover a patient to the receiving hospital, however it is recognised nationally that this has not been met during the year - the average time within our region for 2024/25 was over 38 minutes, however it should be noted that some months exceed this. For example, the average time to handover in January was over 50 minutes.
EEAST has implemented several strategies to reduce ambulance out-of-service times, ensuring quicker responses to emergencies:
Implementation of ambulance handover units
In collaboration with local hospitals, EEAST has introduced ambulance handover units to facilitate quicker patient transfers. For instance, at Southend Hospital, a 12-patient capacity unit was established to expedite handovers, allowing ambulance crews to return to service more promptly. This initiative aims to enhance patient care by ensuring timely medical attention and reducing ambulance turnaround times.
Automatic handover protocols
Working with our hospitals and Integrated Care Systems (ICS) we implemented the system led Handover 45 (HO45) policy in November 2024. This policy, implemented by EEAST and other ambulance services, aims to address delays in transferring patients from ambulances to hospital emergency departments (EDs). Under this policy, if a patient handover is not completed within 45 minutes, ambulance crews may leave the patient in a designated area within the ED, provided the patient is clinically stable. To date, there have been no significant or fatal harm cases reported.
Collaboration with healthcare partners
EEAST collaborates with regulators, commissioners, and hospitals to reduce handover delays. By implementing handover escalation protocols, the organisations work together to identify and address offloading issues promptly, aiming to accelerate care and minimise delays.
Alternative care pathways
To reduce unnecessary hospital admissions and alleviate pressure on emergency departments, EEAST has developed alternative care pathways. These initiatives include the Clinical Assessment Service, which manages a significant proportion of 999 calls through 'hear and treat' methods, providing advice, guidance, or signposting to other services without dispatching an ambulance. Additionally, partnerships with unscheduled care services and the establishment of a single point of contact for referrals to various community services have been implemented. Further information relating to ‘hear and treat’ can be found on the next page.
As well as the Section 64 notification, in January 2025, the Trust also received a Section 29A Warning notice which included concerns regarding our call ‘pick-up’ time and the number of staff within our emergency operations centres (EOCs).
To enable patients to be treated correctly, our Clinical Assessment Service (CAS) continues to develop to ensure that patients who call 999 are directed to the most appropriate care provider for their needs
Following an initial assessment some patients will be managed via our Hear and Treat (H&T) service, this process within ambulance services is provided by paramedics and nurses undertaking enhanced telephone assessments of patients to determine the most appropriate response, which can sometimes result in no ambulance being sent. In May 2024 8.7% of patients were treated through this service, in December 2024 this number had risen to 12% meaning that more ambulances were available for our sickest patients.
Described within last year’s report, C2 segmentation is now part of our business-as-usual process with ongoing work ensuring that as many C2 patients are clinically validated as possible. The number of C2 calls reaching a H&T outcome has averaged between 4% and 6% throughout the year.
Each Integrated Care System (ICS) within the east of England has a functioning Unscheduled Care Coordination Hub (UCCH). Recruitment within each UCCH has resulted in an EEAST clinician co-locating with a multi-disciplinary team within each system every day. This ensures that patient demand of less urgent patients can be managed by the most appropriate community provider. In 2024, a total of 46,864 calls were passed via our Access to the Stack process. Of these, 33,503 (71.5%) were accepted by the community provider for initial management of the patients’ condition (either by telephone or face to face assessment). By working with our partners and allowing them to access our systems supports the Trust’s CAS staff to be able to validate other calls, such as those within the C2 category.
Recruitment within the CAS team has continued throughout the last year. There are now: 113 clinicians,11 clinical workforce managers and 25 clinical navigators all in post, ensuring that that the appropriate structure is in place to provide consistent support to the team and enact the processes to achieve H&T.
Over the next year, the ambition is to increase H&T within the team to 19%. Enablers for this include a continued focus of productivity within the CAS team and ensuring that system collaboration is increased for access to patient pathways.
Heart attack care
Coronary heart disease (CHD; also known as ischaemic heart disease) is the most commonly diagnosed type of heart disease. It is the most common cause of heart attack and is the single biggest killer of both and men and women worldwide. It's also the single biggest premature killer (before the age of 75) in the UK.
As many as 100,000 hospital admissions each year are due to heart attacks. Because of the life-threatening risk with a heart attack, providing patients with a pre-hospital assessment for an ST-elevation myocardial infarction (STEMI) heart attack and administering an appropriate care bundle means a significant improvement on patient outcomes, thereby supporting the NHS to reduce the number of patients dying prematurely and to help people to recover from episodes of ill-health or following injury.
STEMI care bundle
The mandatory quality indicator for ambulance services relating to this topic is the provision of an appropriate care bundle; recording of two pain scores, giving aspirin to break down the clot, giving glyceryl trinitrate (GTN) to dilate the coronary arteries and providing pain relief. The patient care record is audited against all these criteria and deemed to be either compliant or non-complaint.
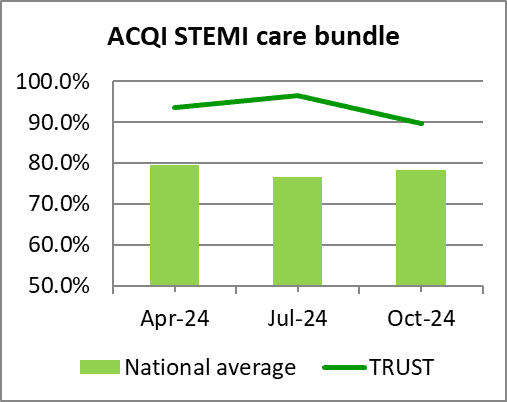
The data is reported on quarterly within the year and the table below shows our result against the national average and the best and worst scores achieved by ambulance services within England.
To provide a robust comparison, the table shows our achievement against the average and upper and lower compliance levels for ambulance trusts that have been published to date (April - October 2024). The graph demonstrates our performance against the national average data for each quarter (April - October 2024), both demonstrating that the Trust is well above the national average for each quarter within the year.
Achieving an average of 93.2% for the year to date, EEAST was the second highest performing Trust for this care bundle achieving 15.0% above the national average.
National data (April to October 2024)
| Heart attack care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| STEMI Care Bundle | 78.2% | 96.1% | 58.2% | 93.2% |
Patients conveyed to a Primary Percutaneous Coronary Intervention (PPCI) Centre
Although the time it takes to transport a STEMI patient to a specialist Primary Percutaneous Coronary Intervention (PPCI) treatment centre is not a quality metric for the Quality Account, we report our achievement on a month-by-month basis to both NHSE and our commissioners. This ACQI contains two joint indicators for ambulance trusts and these centres both of which are measured in hours and minutes.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April – November 2024). It should be noted that the lower score is the best performing score within these outcomes.
Latest data available April – November 2024 hh:mm
| Heart attack care | National average | Upper | Lower | EEAST Performance |
|---|---|---|---|---|
| Mean average time from call to catheter insertion for angiography | 02:30 | 02:55 | 02:20 | 02:33 |
| 90th centile time from call to catheter insertion for angiography | 03:32 | 04:02 | 03:07 | 03:35 |
As shown in the table above, EEAST performed just outside the national average for both of these measures, however we performed significantly higher than the lowest trust.
But, as demonstrated in the previous section, all patients received excellent care, with EEAST consistently achieving high compliance for the STEMI care bundle and being the second highest performing trust within the year.
Next steps
As well as continually being monitored through the national ACQI programme, one of the Trust’s ongoing priorities is to reduce our response times to Category 2 calls which include STEMI patients. This will be supplemented by a local priority for reducing the time spent on scene with these patients which will be monitored through a quarterly audit.
Stroke care - timeliness
Patients who are cared for in a defined stroke unit with organised stroke services are more likely to survive, have fewer complications and return home and regain independence quicker than patients on a general medical ward.
Although the time it takes to convey a stroke patient to hospital is not a quality metric for the Quality Account, we report our achievement on a month-by-month basis to both NHSE and our commissioners. Our performance is assessed monthly against three indicators for this ACQI: the mean average, median and 90th centile times from call to hospital arrival.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April – September 2024). The Lower level relates to the best performing trust for this outcome. Unfortunately, national data reporting from NHS England has paused due to a delay in the implementation of the new Sentinel Stroke National Audit Programme (SSNAP) web tool for submissions so the Trust is unable to benchmark itself against the national average since September.
It should be noted that not all strokes are identified at the time of the call due to the information provided to the call taker, or the patient may deteriorate before or after the crew arrive.
National data – April - September 2024 hh:mm
| Stroke care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| Mean average time from call to hospital arrival | 01:32 | 01:46 | 01:19 | 01:36 |
| Median time from call to hospital arrival | 01:20 | 01:32 | 01:10 | 01:23 |
| 90th centile time from call to hospital arrival | 02:23 | 02:45 | 01:58 | 02:29 |
On average EEAST performed outside the national average for all indicators for this period.
Next steps
As well as continuing to be monitored through the national ACQI programme, one of the Trust’s continuing priorities is to reduce our response times to Category 2 calls which includes stroke patients. This will be supplemented by a local priority for reducing the time spent on scene with these patients which will be monitored through a quarterly audit.
Cardiac arrest care
A cardiac arrest occurs when the heart suddenly stops pumping blood around the body. Someone who is having a cardiac arrest will suddenly lose consciousness and will stop breathing or stop breathing normally. Unless immediately treated by cardio-pulmonary resuscitation (CPR) and early defibrillation, this always leads to death within minutes. It is, however, possible to survive and recover from a cardiac arrest if you get the right treatment quickly. Around two-thirds of cardiac arrests outside of hospital happen in the home, but nearly half of those that occur in public are witnessed by bystanders. With each minute that passes in cardiac arrest before defibrillation, chances of survival are reduced by about 10%.
Although the indicators displayed in the table below are not quality metrics for the Quality Account, we report our achievement on a month-by-month basis to both NHS England and our commissioners, the exception being the post-Return of Spontaneous Circulation (ROSC) care bundle which is a quarterly requirement.
The post-ROSC care bundle contains six components, the recording and administration of: 12 lead ECG; blood glucose; end tidal CO2; oxygen; systolic blood pressure, and saline fluids for all patients who achieve a ROSC on scene which continues to hospital. Patients who had suffered a traumatic cardiac arrest, were successfully resuscitated before the arrival of ambulance staff or were aged less than 18 years are not included.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April – November 2024).
National data – April – November 2024
| Cardiac arrest care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| Return of Spontaneous Circulation (pulse) at hospital– All patients | 27.9% | 31.1% | 19.8% | 30.0% |
| Return of Spontaneous Circulation (pulse) at hospital – Utstein patients | 51.0% | 61.8% | 16.7% | 53.0% |
| Survival to Discharge – All patients | 10.2% | 13.0% | 8.2% | 9.4% |
| Survival to discharge – Utstein patients | 29.8% | 38.1% | 22.8% | 32.4% |
| Post-ROSC care bundle | 83.1% | 97.3% | 75.6% | 97.3% |
Next steps
This will continue to be monitored through the national ACQI programme. Successful outcomes from cardiac arrests are, in part, due to actions taken by acute organisations following arrival at hospital as well as early access to treatment and intervention. As our response times improve, so should our rates of ROSC and survival.
With the exception of 30-day survival (all patients group), EEAST is performing above the national average for all cardiac arrest related indicators. We were the highest performing average compliance for the Post-ROSC care bundle and 14.2% better than the national average for the time period. It should be noted that not all ambulance trusts submitted full data, so these outcomes must be used with caution.
Patient Safety Incidents
A patient safety incident is defined as any unintended or unexpected incident which could have or did lead to harm for one or more patients receiving NHS care. This includes:
- incidents that caused no harm or minimal harm,
- incidents with a more serious outcome,
- prevented patient safety incidents (known as ‘near misses’).
The chart below shows the number of delay incidents vs the total number of patient safety incidents.
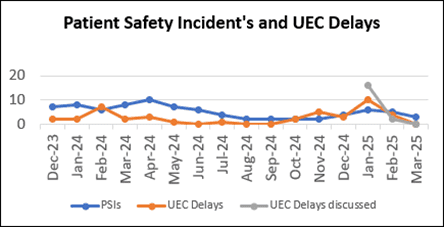
The number of incidents reported by staff during 2024/25 demonstrates a good culture of reporting and being open and honest. Where a near miss has happened, proactive steps can be taken to reduce the risk going forwards and to maintain a learning from incidents culture, the overall number of patient safety incidents relating to delays has decreased since 2022/23 as illustrated in the chart below. The charts below demonstrate our performance for both of these points.
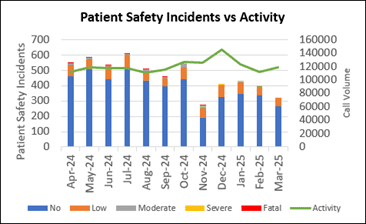
The second chart shows the number of patient safety incidents reported versus our activity during the year.
Prior to the implementation of the Patient Safety Incident Response Framework (PSIRF) EEAST reported on the level of harm they directly caused in relation to individual incidents. Since the implementation of PSIRF in October 2024, the parameters to which levels of harm are reported have been updated in line with Learning from Patient Safety Events (LFPSE) guidance to reflect how EEAST may have contributed towards harm.
A condition within the Quality Account requirements is for each Trust to provide a comparison of their patient safety incidents reported to NRLS against the national average for similar services. However, with this process moving to the new reporting platform, reports have been paused, and no data had been published for 2024/25 at the time of writing this document.
Patient experience and feedback
Although not mandated to report on patient experience, as a Trust we feel that it is important to tell people how we are continually developing and improving our services as a result of our patients’ experiences and feedback. Patients are at the heart of everything we do and as such we believe that the patient voice should be a key driver in the way that we improve our services. The following pages provide information on what our patients and their families have told us through public engagement, complaints, concerns, compliments and surveys, what steps we have taken to improve and how we intend to improve further in the future.
The Patient Experience Team co-ordinate complaints, concerns, compliments and comments as well as leading proactive patient and public engagement for the Trust, in line with the NHS Complaints Regulations 2009, the Public Health Ombudsman Complaints Framework, and local policy. All feedback, both positive and negative, is managed and recorded by the department. Communication with patients or their families is maintained throughout the process, and they are provided with a response to their feedback, with a focus on resolving complaints and identifying learning from both complaints and compliments at the earliest opportunity.
Compliments
Compliments always far outweigh the number of complaints received and in 2024/25, 3,931 compliments were reported to the Trust, which equated to an average of 328 per month (meaning that the average monthly compliments received has consistently increased year on year for the last 3 years). The Trust received four compliments for every complaint received this year (this appears lower than last year due to changes in the way that the Trust now records complaints as described below). Compliments are reported to the Trust board and the individual colleague and are recorded on the staff member’s personnel file. This year we have started looking at themes from compliments to help us learn from excellence, and the common themes include professionalism, kindness and being calm and reassuring.
| Apr-24 | May-24 | Jun-24 | Jul-24 | Aug-24 | Sep-24 | Oct-24 | Nov-24 | Dec-24 | Jan-25 | Feb-25 | Mar-25 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Compliment | 365 | 331 | 280 | 382 | 331 | 358 | 296 | 296 | 305 | 317 | 293 | 377 |
| Complaint | 89 | 69 | 90 | 103 | 84 | 74 | 79 | 72 | 50 | 47 | 55 | 44 |
Complaints
As a Trust we closely monitor the numbers and themes of complaints that we receive and use this learning to support service improvement. During 2024/25, in order to comply with the Public Health Ombudsman Complaint Framework Guidelines, expressions of dissatisfaction ceased being categorised into complaints and concerns, with all being recognised and reported as a complaint. This means that the overall number of complaints this year is higher than previous years at 868, however when compared to the total number of complaints and concerns combined last year, we see a reduction.
Complaints arose from 0.05% of our contacts with patients which is a sustained improvement of 0.1% on the previous year. All complaints which cannot be resolved under early resolution receive a local investigation and depending on the nature of the complaint or concern, may also be reviewed by the patient safety team. Complainants are supported through the process of raising a complaint and investigation by our patient experience coordinators, and upon receiving a written response, face to face meetings are arranged where complainants require further support. An anonymous sample of our complaint responses is reviewed by the Trust volunteers from the Community Engagement Group and feedback is provided to the patient experience team to ensure improving quality of complaints.
The number of re-opened complaints remains very low (1.2% of all complaints responded to this year), meaning complainants are usually satisfied that our responses have addressed and where able, resolved their questions and concerns.
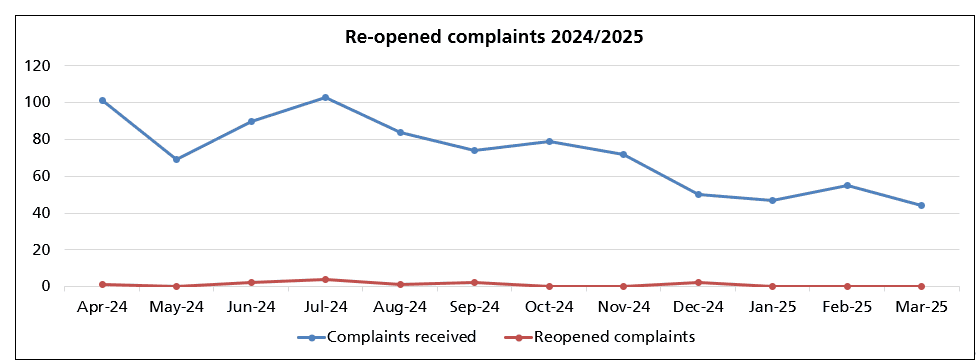
Graph showing the number of compliments and complaints received each month during the year.
The biggest theme from complaints and concerns was delay, with most of those complaints (62%) being related to The Patient Transport Service (PTS) rather than Urgent and Emergency Care (UEC) service or our Emergency Operations Centres (EOC). The next biggest themes were transport and driving (88% of these complaints were for PTS), attitude which largely related to the Trust’s UEC service (76% of complaints were for our UEC service), and clinical assessment and treatment (which by nature relates almost entirely to our UEC services and emergency operations centres). It is of note that although the themes of complaints remain the same, progress is demonstrated by the reduction in numbers of complaints received in most of these areas. Delay complaints were reduced by 30% compared to 2023-2024 with reductions in all services but the most significant reductions for PTS. Similarly transport and driving complaints were reduced by 12% compared to the previous year, with the reduction almost entirely in PTS. Clinical assessment and treatment complaints, which largely relate to UEC services and EOC decreased by 21% on the previous year.
These reductions in complaints represent improvements in emergency ambulance attendance times achieved via the Trust’s delay action plan and in the last quarter of the year, through interventions such as the implementation of handover in 45 minutes with local acute hospitals. Regarding clinical assessment and treatment, reductions in complaints are likely to also reflect an increase in admission avoidance schemes, increased out of hospital treatment options and pathways and internal learning from Patient Safety Incident Reviews. For the patient transport service, reductions in complaints are the likely result of improvements to their planning and prioritisation of service delivery as well as the cessation of one of their most over utilised contracts.
Parliamentary and Health Service Ombudsman (PHSO)
Although most complaints are successfully resolved through the Trust’s complaints process, complainants can refer their complaint to the Parliamentary and Health Services Ombudsman (PHSO) for an independent review. This happens if a complainant feels that their complaint has not been resolved, and the Trust has exhausted all avenues of resolution. This provides complainants with an impartial, independent review of their complaint and gives clear guidance to the Trust on how to improve our investigations and responses.
In 2024/2025 the Trust was not notified of any cases which had been referred to the PHSO by complainants. We do still have complaints in initial review from 2023/2024, although the Trust has not yet received initial feedback indicating whether these will move to an investigation. The Trust was notified this year that the PHSO did partially uphold two complaints from 2023/2024. Given the length of time since these complaints had been made, the Trust had already implemented learning by the time that the PHSO notifications were received.
You said, we did
As a Trust we recognise the importance of learning when things have not gone as well as we would have liked or from our patient survey feedback. The following case studies are just three examples of some of the learning from last year.
| You said | What we did | What this means |
|---|---|---|
| We were receiving frequent complaints that our Patient Transport Services were cancelling lots of appointments at the last minute, and that patients felt that organisation was poor. | We invested in upgraded software which allows the control room to plan journeys six weeks in advance. The letters to patients who have experienced delays and cancellations have been worked on to include information about the challenges that the service is facing and the agreements for prioritising patients where demand exceeds capacity. | Where journeys have been over booked, in most cases patients have sufficient time to make alternative transportation arrangements rather than having to cancel their appointments. Where patients have still had poor experiences, our letters are more transparent about the challenges facing the service, the plans in place to reduce these and what this may mean for their care. |
| Patient feedback from the Stroke video triage project said that patients were pleased to have received a video triage assessment and with the outcome of this. | As a result of this and staff feedback, we have worked with local hospitals to increase the times that this is available and to implement stroke video triage in more hospitals. Survey feedback has been shared nationally and internationally as part of ongoing research into stroke video triage. | More patients within EEAST’s region will be able to benefit from the reduced arrival to images and intervention times that the stroke video triage project has already demonstrated. Patient feedback and EEAST’s work on this is contributing to improving the stroke pathway for the ambulance sector nationally. |
| Patients in the 16-24 age group have consistently said that they are less happy with the services that they receive from EEAST than other age groups. | We have amended our safeguarding policies, developed policies around parental involvement and explored solutions to practical barriers to allow 16- and 17-year-olds to volunteer for the Trust Community Engagement Group. | We anticipate our first 16- and 17-year-old volunteers being able to join the Trust in 2025. This will mean that this age group is better represented and has more opportunity to contribute directly towards service improvement. |
Patient surveys
As stated within a previous section, the Trust has a comprehensive annual patient survey programme which includes continuous surveys for the urgent and emergency care service (UEC) and the patient transport service (PTS).
Patient surveys are signposted using a variety of methods, including the Trust’s social media channels, invitation to feedback letters and patient information cards. In addition, 60.0% of PTS survey submissions received during 2024/25 have resulted directly from SMS signposting.
Listening to the patient voice enables the Trust to identify, not only what is working well, but also to highlight areas for learning and service improvement. Feedback received through surveys is monitored and triangulated with the themes identified through complaints, patient engagement, and patient safety to ensure appropriate governance, learning, and to improve patient experience and outcomes.
It also enables the Trust to identify areas of excellence and highlight areas for learning and service improvement. Feedback received through surveys is continually monitored and triangulated with the themes identified through complaints, patient engagement, and patient safety to ensure appropriate governance, learning and to improve patient experience and outcomes.
All patient surveys include the Friends and Family Test (FFT) question, ‘Overall, how was your experience of our service?’ The FFT is a method of calculating the overall satisfaction of the patient and is used as a benchmark across the Trust. The FFT result is calculated by dividing the proportion of ‘very good’ and ‘good’ responses (numerator), by the overall number of responses (denominator).
The FFT is a national directive, and the Trust is required to provide all PTS patients with the opportunity to respond to the FFT question, with results reported monthly to NHS England.
Outcomes from 2023/24 and 2024/25 can be found below. Historically, survey feedback demonstrated higher satisfaction levels for EUC patients, however, recent years have seen UEC and PTS patient satisfaction to have become more comparable.
Overall Satisfaction (Friends and Family Test)
| Continuous Patient Survey Results: | Number of patients: 2023/24 | Overall Satisfaction: 2023/24 | Number of patients: 2024/25 | Overall satisfaction: 2024/25 |
|---|---|---|---|---|
| Urgent and Emergency Care | 873 / 978 | 89.3% | 702 / 815 | 86.1% |
| Patient Transport Service | 1180 / 1401 | 84.2% | 1612 / 1865 | 86.4% |
| All Services | 2053 / 2379 | 86.3% | 2314 / 2680 | 86.3% |
Survey projects
This section provides further information on each of the surveys undertaken throughout the year.
Easy Read
The easy read survey (co-produced with the D.R.A.G.O.N.S at the Norfolk and Norwich SEND Association (NANSA) has remained available as an accessible survey option for UEC and PTS patients, empowering patients to provide feedback on their experiences to drive forward learning, improvement and informed decision making.
Feedback received during 2024/25 has generally been positive about the service and staff (overall satisfaction: 92.6%). Most patients felt listened to (96.2%), with staff communicating in an understandable way (98.1%), ensuring any sensory needs were met. The main area of dissatisfaction has related to ambulance and PTS delays, which has been shared as part of the ongoing wider system review.
This survey has highlighted the importance of co-production and working in equal partnership with experts by experience. Building on the co-production sessions, a short video was created to explain how to complete the survey and to outline how feedback is used. The video, which includes a British Sign Language (BSL) translator and voiceover (recorded by a NANSA D.R.A.G.O.N), is now available to view on the EEAST website.
Safeguarding
The safeguarding survey has continued throughout 2024/25, with the aim being to obtain feedback from patients who had consented to a safeguarding referral (e.g. mental health services, falls team, GP, local authorities and the Fire and Rescue Service).
Overall satisfaction levels have remained high (96.3%), with patients generally advising that they were included in discussions relating to their referral and support needs (88.1%).
Just under three quarters of patients surveyed (71.8%) went on to receive additional support post referral. Dissatisfaction has mostly related to delays and communication.
Patient feedback received has been utilised as an assurance tool, and during 2024/25, survey findings have also been shared within the CQC Joint Targeted Area Inspections of Hertfordshire County Council and Norfolk County Council, Safeguarding Adult Boards and Safeguarding Care Act audits across the region. EEAST has taken the lead in being able to demonstrate this level of engagement.
The safeguarding survey will be undertaken again during 2025/26 to measure impact on patient experience considering the impending changes relating to the introduction of electronic safeguarding referrals (via iPads rather than Single Point of Contact (SPOC) contact).
Maternity
The maternity survey has continued as an online option during 2024/25, enabling patients to provide feedback following their maternity related 999-emergency call.
Whilst patients have continued to mostly report a positive experience of the staff and service received (94.1%), several patients expressed dissatisfaction with the advice provided, prompting suggestions relating to additional obstetric training for both clinicians and call handlers. This has been shared with the maternity lead and specialist midwife to ensure learning and further training as required e.g. videos (such as for delayed cord clamping).
Stroke video triage
During 2024/25, the stroke video triage survey has continued to proactively seek feedback from patients who received a pre-hospital stroke video triage assessment, with this initiative in place to ensure timely, appropriate care and the best possible patient outcome. The pathway itself has had a positive impact on patient arrival to imaging time, alongside significant reductions in the treatment times for stroke at all live centres.
Survey feedback has also demonstrated that patients have generally been satisfied with the service received (80.4%) and pleased to have received a video triage assessment. The slightly lower than expected satisfaction level generally relates to many patients being unaware that an assessment had been undertaken using this method – promoting the need for improved communications. Aside from ambulance response times, areas for improvement also related to WIFI connectivity and the need to extend the availability of this virtual method.
Survey feedback has been shared widely, including NHS England, the Integrated Stroke Delivery Network, both national (UK Stroke Forum) and international (European Stroke Organisation Conference) conferences, and as part of ongoing research looking at the experiences of patients and caregivers involved in stroke video triage.
These opportunities have successfully raised the profile of EEAST, whilst evidencing the efficacy of the project to improve patient experience, outcomes and optimisation of the stroke pathway for the ambulance sector nationally.
Mental health
During 2024/25, two co-produced Instagram poll surveys relating to mental health have continued to obtain feedback from patients who had contacted 999 when experiencing a mental health crisis.
Whilst feedback has continued to demonstrate satisfaction with the service received from EEAST (between ‘good’ and ‘very good’ on the sliding scale), feedback continues to highlight the need for improved mental health support and signposting. In addition, approximately a quarter of patients have advised that they did not feel listened to or understood by the emergency call handler. Patients have also continued to stress the importance of only telling their story once.
The survey feedback has been shared widely to ensure 360 feedback, working with mental health practitioners, commissioners, partner organisations and experts by experience to ensure system wide learning and improvements to the service provided to patients.
As a result of patient feedback;
- further co-produced call handler engagement sessions are in development for 2025/26.
- 999 emergency pathway videos and infographics are now available on the public website.
- In addition, the summer engagement programme will focus on education relating to the clinical model and the importance of the right care, by the right person, at the right time.
Admission avoidance
This year has seen the undertaking of several admission avoidance related surveys, with a view to proactively obtain feedback from patients who received assessment/treatment within the home setting, with many avoiding conveyance to hospital.
Admission avoidance initiatives aim to ensure the right care, by the right person, at the right time – with survey feedback received demonstrating positive patient experiences and outcomes, with demand upon acute Trusts also reduced as a result.
Surveys have related to skin tear wound treatment, the Physician Response Unit pilot and the Advanced Practice Team. Patients have largely supported such models of care, with many thankful to have avoided the need for hospital admission and associated handover delays.
Areas of dissatisfaction have generally related to delays and communication, although these comments have been in the minority. In addition, it is clear from feedback received that patients are not always aware of/understand the range of services and possible outcomes following emergency call triage.
The collation of patient feedback provides tangible evidence of satisfaction, effectiveness and outcomes. This is crucial to refine services and secure longer-term funding and wider implementation post pilot. This year’s engagement programme will also focus on education relating to the clinical model and alternative pathways in place.
Next steps
The Trust is committed to developing its patient experience and engagement activity and continually explores new methods to obtain feedback and to ensure equity of care across the demographics, including seldom heard groups.
During 2025/26, there will be a focus on expanding the Community Engagement Group, with a view to diversify the group, and encourage younger engagement across the region.
Co-production and working with experts by experience will continue to be embedded as standard practice, placing our patients and communities at the heart of service design, development and evaluation.
In addition to the continuous surveys, the 2025/26 survey programme will include several planned projects, with a prioritisation on learning and improvement - ensuring incorporation of the Trust priorities and the Patient and Public Involvement strategic objectives. Key survey results and themes will continue to be reported as part of the internal and external quality and assurance reporting channels, ensuring the patient voice is at the heart of the organisation.
Commissioning for Quality and Innovation (CQuIN)
The CQuIN scheme is intended to deliver clinical quality improvements and drive transformational change and will impact on reducing inequalities in access to services, the experiences of using them and the outcomes achieved. Our CQuINs are agreed with our commissioners as part of our contract negotiations and have traditionally been a mix of nationally mandated and locally determined Quality and Service Delivery Improvement Programmes.
Since the Covid-19 pandemic CQUIN deliverables were largely suspended by NHS England which have not yet been re-instated
As such, there were no locally determined CQUINs in 2024/25 and the only national CQUIN for Ambulance Services related to the uptake of the flu vaccine, as there is each year in support of the protection against infectious illness. EEAST, achieved 33% for all directly employed staff which is considerably lower than achievements in previous years.
Although 39% of UEC operations staff did receive this, uptake was much lower among other staff groups.
Several lessons have been learned for the 2025/26 vaccination programme with four key improvement areas identified:
- Incentives – to encourage staff to be vaccinated.
- Vaccinator lead role – to ensure effective coordination of clinics, stock and vaccine fridges
- Bespoke software – to improve the process for appointments, reminders and to generate reports.
- Utilising welfare wagons – to improve accessibility for staff.
Poster displayed on our premises to encourage staff to receive vaccinations.

